How antibody-drug conjugates became oncology's hottest therapeutic class
Few areas of oncology have advanced as quickly as antibody-drug conjugates. Once regarded as an ambitious, sometimes controversial, and technically challenging concept, ADCs are now a staple feature of treatment across multiple cancer types, with new approvals and innovations continuing to expand their role on a near-daily basis.
Yet, despite their importance in modern oncology, just a few years ago, ADCs looked set to become a mere footnote in the history of failed cancer treatments. So, how did this groundbreaking concept survive more than a century of clinical setbacks, scientific criticism, and technological limitations to become the “magic bullet” reality we have today?
1900s
The story of ADCs began nearly a century ago – in the mind of an infamous German scientist and Nobel laureate, whose name has become synonymous with two defining treatments in oncology.
At the turn of the 20th century, in a country that no longer exists, Dr Paul Ehrlich occupied his working days studying the therapeutic properties of chemical dyes. As he methodically pipetted droplets of liquid onto different tissue samples, he began to notice an unusual pattern. Not all dyes behaved the same way. Some would stain certain cells, but leave others completely untouched. Others would stain only a specific part of a cell. It was, he theorised, as if they had a built-in roadmap telling them where to go.
Using his foundational knowledge of chemistry, Ehrlich reasoned that, in the same way that dye molecules were known to have side chains related to their colouring properties, living cells must also have these ”side chains” that would break off and hunt down toxins. It was these toxin-hunting antibodies that gave life to Ehrlich’s theory, Zauberkugel, or "magic bullet” for those who don’t speak German.
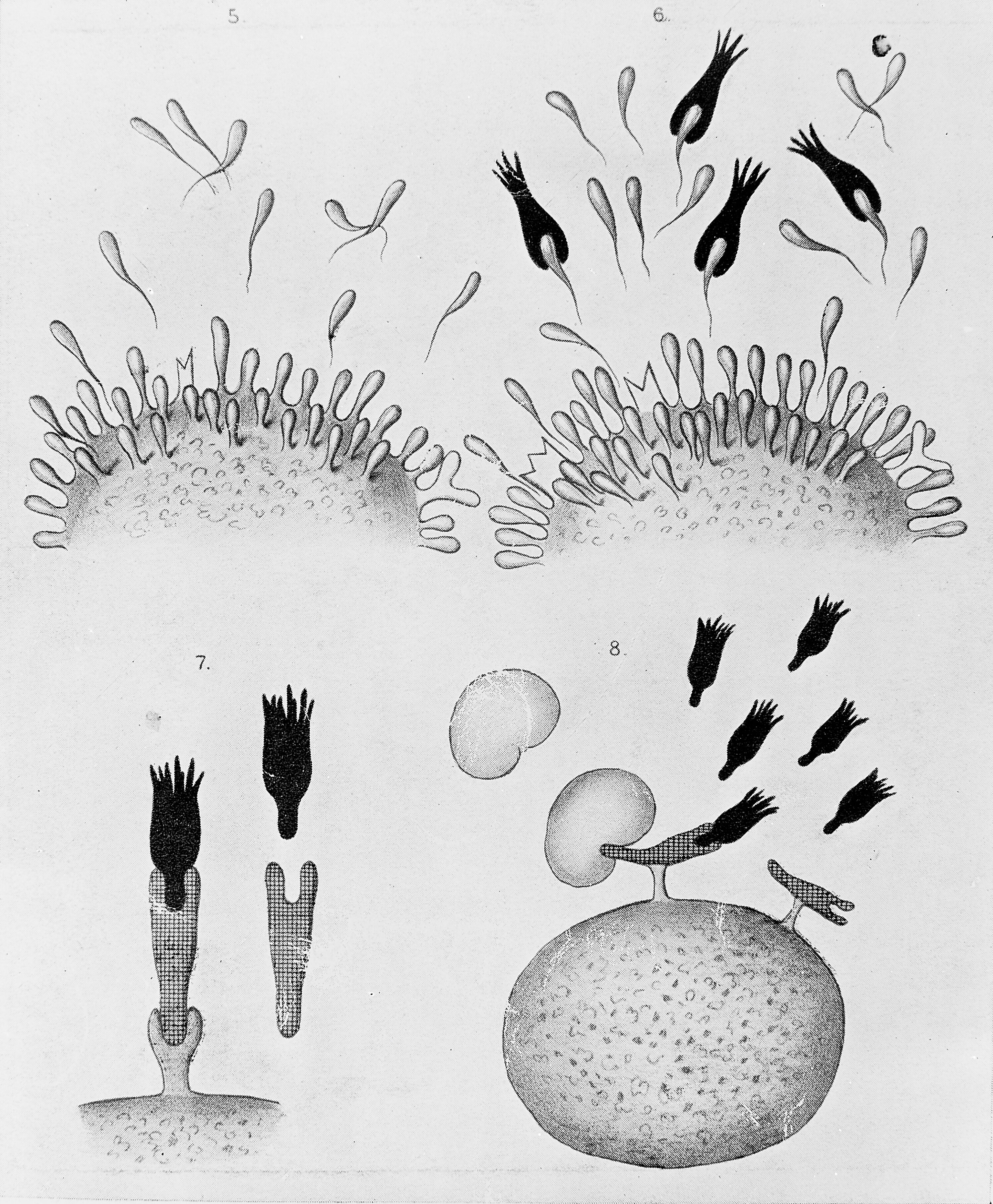
Diagram illustrating the side-chain theory of Paul Ehrlich. Source: Wellcome Collection
This simple observation sparked what would become a lifelong obsession for Ehrlich. If nature could create such precision-guided weapons, he reasoned, surely scientists should be able to engineer their own.
Unfortunately, as is often the case in history, such a radical departure from the blunt-force approaches that characterised much of medicine at the time wasn’t well received by his contemporaries – most notably the Austrian Dr Max Von Gruber, who, in 1901, launched a two-year polemic against Ehrlich’s theory. He published highly critical, and often inexcusably insulting, papers denouncing Ehrlich's models – particularly his side-chain hypothesis.
Ehrlich's first attempt to turn theory into practice came in 1910 with Salvarsan, a syphilis treatment known as "606". While the drug was an immediate sensation, becoming one of the most widely prescribed medicines in the world, its success was once again marred by controversy. Salvarsan was denounced by some physicians as too difficult to administer and associated with too many significant side effects, including rashes and liver damage. What’s more, in what historians later termed the "Salvarsan Wars", Ehrlich and his co-creator, Dr Sahachirō Hata, faced accusations of profiteering and criminal negligence before ultimately being cleared of wrongdoing.
Despite the turmoil, the underlying principle that a therapeutic agent could selectively find and destroy diseased cells endured in a curiosity that researchers would spend decades exploring (as well as an Oscar-nominated movie).
1970
By the 1970s, scientists had successfully mapped the molecular structure of antibodies. Thanks to advancements in both biology and technology, they could now produce antibodies by injecting a target antigen into an animal and harvesting the diverse array of antigens produced by the animal's immune system. The problem was that the resulting antibody mixtures – known as polyclonal antibodies - lacked specificity and batch-to-batch uniformity, making it difficult to replicate experiments or compare results.
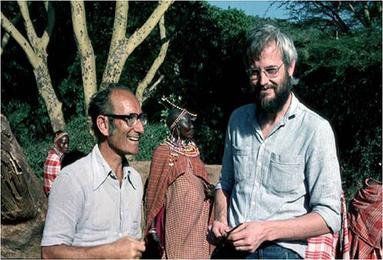
Pictured::César Milstein and Georges Köhler. Source: Wikimedia Commons
{kind=link}
The solution to that problem was found in the MRC laboratory of molecular biology in Cambridge, UK, where, in 1975, post-doctoral fellow Georges Köhler and then-28-year-old Argentinian chemist César Milstein were hunting for a way to generate antibodies of a single defined specificity.
By immunising a mouse with a target antigen, isolating antibody-producing B lymphocytes from the spleen, and fusing these short-lived cells with immortal myeloma cells, Köhler and Milstein discovered that they could create hybrid cells, later known as hybridomas, that could divide indefinitely while continuously producing one highly specific monoclonal antibody. For the first time, researchers could create antibodies that reliably recognised a chosen target – a prerequisite for any future ADC. For their findings, the pair would be jointly awarded the Nobel Prize for Physiology or Medicine in 1984.
1980-1990
Armed with this breakthrough, scientists began testing some of the first experimental ADCs in the 1980s. Early attempts linked antibodies to highly potent cancer drugs, but the results exposed significant challenges, including unstable linkers, toxic payloads that detached before reaching their targets, and unintended immune reactions. The promise was evident, but just as Dr Ehrlich had found, the technology wasn’t ready to realise it.
At the same time, researchers were uncovering new cancer targets. In 1984, scientists identified the HER2 gene, while three years later Dennis Slamon demonstrated its critical role in a significant proportion of breast cancers.
Moreover, advancements in antibody engineering and linker chemistry steadily improved the field's prospects throughout the 90s, leading to landmark approvals of monoclonal antibodies such as rituximab in 1997 and trastuzumab in 1998. While neither was an ADC, they provided solid proof that targeted biological therapies could succeed in the clinic.
2000
After decades of dedicated research building toward the first ADC approval, anticipation was at an all-time high in 2000 when the US Food and Drug Administration green-lit accelerated approval for the first of its kind, gemtuzumab ozogamicin (marketed as Mylotarg by Wyeth) for patients with CD33-positive acute myeloid leukaemia (AML). At long last, Ehrlich's century-old vision of a targeted “cancer killing” therapy had been realised.
Unfortunately, the success story would quickly become a cautionary tale for the industry.
The problems began early. Traditional FDA approvals required randomised, controlled trials showing solid safety and efficacy results against a disease. But, because Mylotarg was the first AML drug to be brought to market in 15 years, it met the criteria for accelerated approval, which required a lower standard of proof before approval – most notably, there was no empirical evidence that the drug improved survival rates.

While Wyeth worked to get a required post-market Phase 3 study off the ground, around the world, independent research groups launched their own studies to test the validity of the ADC in different doses and populations. The results were not good. Clinical studies linked the drug to serious toxicities and, in an unexpected blow to the development team, showed that the treatment failed to demonstrate a clear clinical advantage over standard therapies.
The fallout was swift. Pfizer, which had acquired Wyeth – and by association Mylotarg – in 2009, was forced to pause its Phase 3 trial, as the FDA pushed for gemtuzumab ozogamicin to be withdrawn from the market. In June 2010, Pfizer relented and voluntarily pulled the plug on Mylotarg (for now, at least).
2011
While Mylotarg's withdrawal appeared to cast doubt on the future of ADCs, the drug had left a legacy that was difficult for researchers to ignore: selective delivery of highly potent cytotoxins to cancer cells was clinically achievable.
And so, undeterred by this minor setback, researchers used the lessons of gemtuzumab ozogamicin to refine every component of ADC design - from the antibodies themselves to the chemistry linking them to their cytotoxic payloads.

The first signs that those lessons were paying off arrived in 2011 with the approval of Brentuximab vedotin (Adcetris) for relapsed or refractory Hodgkin lymphoma and systemic anaplastic large cell lymphoma. Developed by Seattle Genetics (now Seagen) and Takeda, the treatment targeted the CD30 protein using a monomethyl auristatin E (MMAE) payload connected by a protease-cleavable linker that would release the agent upon internalisation into CD30-expressing tumour cells, but remain stable in the blood.
2013
A second milestone followed just two years later. In 2013, ado-trastuzumab emtansine (Kadcyla) gained approval for HER2-positive breast cancer. The culmination of decades of research into HER2 biology and the foundation of success laid by trastuzumab, Kadcyla became the first ADC approved for a solid tumour, further demonstrating the promise of ADCs beyond liquid tumours.
2015-2016
By the second half of the 2010s, ADCs had evolved from a promising niche technology into one of the most closely watched areas in oncology.
Among the many advancements in ADC research during these five years, perhaps the most transformative was the emergence of topoisomerase I (TOP1) inhibitor payloads. Unlike earlier, highly toxic payload classes, these potent compounds enabled researchers to achieve safer, more precise release inside cancer cells, giving rise to a new generation of therapies, including trastuzumab deruxtecan (T-DXd), datopotamab deruxtecan, and acituzumab govitecan.
2017
After seven years in exile, it was time for a familiar name to make a long-awaited comeback. In September 2017, gemtuzumab ozogamicin officially returned to the market, having secured re-approval for the treatment of adults with newly diagnosed CD33-positive AML, as well as the treatment of patients aged two years and older with CD33-positive relapsed/refractory AML. Only, this time, the drug came with revised dosing schedules and a better understanding of how to manage its risks.
2019-2020
In 2019, a flurry of new approvals, including enfortumab vedotin (brand name, Padcev) and polatuzumab vedotin (Polivy), expanded the reach of ADCs into new disease settings and validated additional molecular targets.

Later that year, trastuzumab deruxtecan (Enhertu), developed by AstraZeneca and Daiichi Sankyo, received accelerated approval for previously treated HER2-positive metastatic breast cancer. With its sophisticated design, comprising a high drug-to-antibody ratio, tumour-selective linker, and membrane-permeable payload capable of generating a bystander effect, Enhertu quickly established a new benchmark for ADC performance, generating approximately 2.8 billion to 3.8 billion annually.
This momentum continued into 2020 with the approval of Gilead’s sacituzumab govitecan, under the brand name Trodelvy, further reinforcing the growing role of ADCs in solid tumours.
By 2021, there were 11 FDA-approved ADC products, with a combined market size projected at $16.5 billion by 2030.
2021
By the early 2020s, ADCs had become one of the most promising areas in oncology, attracting billions of dollars in partnerships, acquisitions, and research programmes as companies raced to secure a position in what many viewed as the next frontier of precision medicine.
Much of this excitement was driven by the stand-out success of trastuzumab deruxtecan. Building on its initial approval, the therapy continued to redefine the status quo of cancer treatment with new data across multiple settings, fuelling heightened interest in HER2-directed conjugates and the broader application of the platform.

In 2021, Genmab and Pfizer’s tisotumab vedotin (Tivdak) expanded the use of ADCs into additional solid tumour settings, while advances in linker stability, site-specific conjugation techniques, and novel payloads accelerated the development of an increasingly diverse pipeline.
2024
For much of their development, ADCs were evaluated one at a time. But, in 2024, that approach shifted with the publication of the first Dual ADC (DAD) trial, combining enfortumab vedotin and sacituzumab govitecan. In the study, researchers sought to understand whether two ADCs with different targets could be given together, a question that challenged commonly held beliefs that combining ADCs would compromise safety. Results, presented at ESMO 2023, revealed the opposite: a 70% objective response rate in treating heavily pretreated, metastatic urothelial carcinoma.
2025
Having cemented its reputation in the ADC landscape, Enhertu added a number of important notches to its belt in 2025, including positive results in early breast cancer, and then in the 'post-neoadjuvant' setting, as well as approvals in Europe for use in advanced breast cancer cases with lower levels of the HER2 biomarker, and FDA approval in combination with pertuzumab.
Clinical progress was accompanied by commercial expansion. Large pharmaceutical companies continued to invest heavily in ADC development, while regulatory approvals broadened the range of cancers in which the drugs could be used.
2026
Twenty-five years after the first ADC was approved, the field looks markedly different. More than a dozen conjugates are now available across haematological malignancies and solid tumours, with hundreds more in development. Moreover, current research is looking for ways to refine the approach by identifying the right patients, understanding resistance, reducing toxicity, and developing new payloads and linker technologies.
However, progress is not always a straight line, as Pfizer recently discovered when one of the ADCs at the heart of its $43 billion Seagen acquisition failed to meet its primary endpoint in a phase 3 trial. Meanwhile, others are celebrating new wins, such as Astellas' Padcev and Gilead's Trodelvy, which claimed new approvals in bladder cancer and triple-negative breast cancer, respectively, from the EMA in June.
It’s a mixed bag of results, but looking at how many developments - both good and bad - are emerging in the ADC space gives us the clearest indication of how far the field has come in a few short years.

About the author
Eloise McLennan is the editor for pharmaphorum’s Deep Dive magazine. She has been a journalist and editor in the healthcare field for more than five years and has worked at several leading publications in the UK.
Supercharge your pharma insights: Sign up to pharmaphorum's newsletter for daily updates, weekly roundups, and in-depth analysis across all industry sectors.
Want to go deeper?
Continue your journey with these related reads from across pharmaphorum
Five dynasties that built modern pharma

GLP-1s: Five years that changed metabolic medicine

A history of vaccination: How immunisation transformed public health
The AI drug discovery race: Who’s leading the charge?


Click on any of the images below for more articles from this edition of Deep Dive: Oncology 2026
.jpg)
.jpg)
.jpg)

.jpg)
.jpg)